

Double Your Impact on Millions of Lives
Double Your Impact on Millions of Lives
Now is the time to do more in the fight against Alzheimer’s and all other dementia. Give by July 20 and your gift can be matched, up to $35,000, to fund research that is helping protect brain health and provide care and support.
Donate NowParkinson's Disease Dementia
Parkinson's disease dementia is a decline in thinking and reasoning skills that develops in some people living with Parkinson’s at least a year after diagnosis.
About Parkinson's disease dementia

Parkinson’s disease dementia is a decline in thinking and reasoning skills that develops in some people living with Parkinson’s at least a year after diagnosis. The brain changes caused by Parkinson’s disease begin in a region that plays a key role in movement, leading to early symptoms that include tremors and shakiness, muscle stiffness, a shuffling step, stooped posture, difficulty initiating movement and lack of facial expression. As brain changes caused by Parkinson’s gradually spread, the person may also experience changes in mental functions, including memory and the ability to pay attention, make sound judgments and plan the steps needed to complete a task.
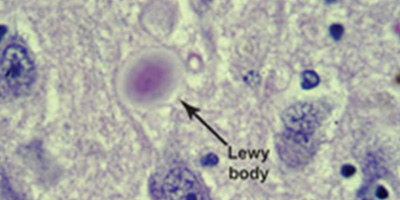
The key brain changes linked to Parkinson’s disease and Parkinson’s disease dementia are abnormal microscopic deposits composed chiefly of alpha-synuclein, a protein found widely in the brain whose normal function is not fully understood. The deposits are called “Lewy bodies” after Frederick H. Lewy, M.D., the neurologist who discovered them while working in Dr. Alois Alzheimer’s laboratory during the early 1900s.
Lewy bodies are also found in other types of dementia, including dementia with Lewy bodies (DLB). Evidence suggests that DLB, Parkinson’s disease and Parkinson’s disease dementia may be linked to the same underlying abnormalities in the brain processing of alpha-synuclein. Another complicating factor is that many people with both Parkinson’s disease dementia and DLB also have plaques and tangles — hallmark brain changes linked to Alzheimer’s disease. When evidence of more than one type of dementia is found in the brain, it is called mixed dementia.
A study published on July 29, 2019 in Scientific Reports suggests that Lewy bodies are problematic because they pull alpha-synuclein protein out of the nucleus of brain cells. The study, which examined the cells of living mice and postmortem brain tissue in humans, reveals that these proteins perform a crucial function by repairing breaks that occur along the vast strands of DNA present in the nucleus of every cell of the body. Alpha-synuclein's role in DNA repair may be crucial in preventing cell death. This function may be lost in brain diseases such as Parkinson's and DLB, leading to the widespread death of neurons.
Learn more: Dementia with Lewy Bodies and Mixed Dementia.
Prevalence
Parkinson’s disease is a fairly common neurological disorder in older adults, estimated to affect nearly 2% of those over age 65. The Parkinson’s Foundation estimates that nearly one million Americans are living with Parkinson’s disease. This is expected to rise to 1.2 million by 2030.
Causes and risk factors
Some studies have reported that the average time from onset of Parkinson’s to developing dementia is about 10 years. One large study found that about three-quarters of people who live with Parkinson's for more than 10 years will develop dementia. Before they develop dementia, they experience milder cognitive changes called mild cognitive impairment (MCI). Among individuals with normal cognition at Parkinson's diagnosis, about 30% will develop MCI after five years. However, cognitive changes and when they occur vary from person to person.
Certain factors at the time of Parkinson’s diagnosis may increase future dementia risk, including advanced age, greater severity of motor symptoms and mild cognitive impairment.
Additional risk factors may include:
- The presence of hallucinations in a person who doesn’t yet have other dementia symptoms.
- Excessive daytime sleepiness.
- A Parkinson’s symptom pattern known as postural instability and gait disturbance (PIGD), which includes “freezing” in mid-step, difficulty initiating movement, shuffling, problems with balancing and falling.
Symptoms
Commonly reported symptoms include:
- Changes in memory, concentration and judgment.
- Trouble interpreting visual information.
- Muffled speech.
- Visual hallucinations.
- Delusions, especially paranoid ideas.
- Depression, irritability and anxiety.
- Sleep disturbances, including excessive daytime drowsiness and rapid eye movement (REM) sleep disorder.
Diagnosis
There is no single test — or combination of tests — that conclusively determines that a person has Parkinson’s disease dementia. Guidelines for diagnosing Parkinson’s disease dementia and DLB are:
-
The diagnosis is Parkinson’s disease dementia when a person experiences dementia at least one year (and usually several years) after the onset of symptoms of Parkinson’s disease. Parkinson's disease symptoms may include changes in movement like a tremor.
-
The diagnosis is DLB when a person experiences dementia either before, at the same time as, or within one year of the onset of symptoms of Parkinson’s disease. In some cases of DLB, symptoms of Parkinson’s disease, like changes in movement, may never occur.
Outcomes
Because Parkinson’s disease and Parkinson’s disease dementia damage and destroy brain cells, both disorders worsen over time. Their speed of progression can vary widely.Treatment
There are no treatments to slow or stop the brain cell damage caused by Parkinson’s disease dementia. Current strategies focus on improving symptoms. If your treatment plan includes medications, it’s important to work closely with your physician to identify the drugs that work best for you and the most effective doses.
- Cholinesterase inhibitors — drugs that are the current mainstay for treating cognitive changes in Alzheimer’s — may help Parkinson’s disease dementia symptoms, including visual hallucinations, sleep disturbances and changes in thinking and behavior.
- Carbidopa-levodopa — may be prescribed to treat Parkinson's movement symptoms. However, it can sometimes aggravate hallucinations and confusion in those with Parkinson's dementia or DLB.
- Deep brain stimulation — deep brain stimulation (DBS) is currently contraindicated for Parkinson’s disease dementia (PDD). Although one small clinical study suggested it was safe for those with PDD, additional studies must be conducted to confirm its effectiveness.
- Selective serotonin reuptake inhibitors (SSRIs) — used to treat depression, which is common in both DLB and Parkinson’s disease dementia.
- Clonazepam and melatonin — may be used to treat REM disorder.
Caution: Antipsychotics drugs (such as haloperidol, fluphenazine or thioridazine) that are used to treat behavioral symptoms should be avoided. About 60 percent of people with DLB who receive antipsychotic drugs experience worsening of Parkinson's symptoms, sedation, impaired swallowing or neuroleptic malignant syndrome (NMS). NMS is a life-threatening condition characterized by fever, generalized rigidity and muscle breakdown.
Help is available
The Alzheimer's Association can help you learn more about Alzheimer's disease and other dementias, and help you find local support services. Call our 24/7 Helpline at 800.272.3900.
Michael J. Fox Foundation for Parkinson's Research website offers information for people living with Parkinson's disease and research updates.
Parkinson's Foundation is a nonprofit organization providing information and resources for diagnosed individuals, families and health professionals. Call the Parkinson's Foundation at 800.473.4636.
Related Pages



The Alzheimer’s Association is in your community.
Find Your Local Chapter
Learn how Alzheimer’s disease affects the brain.
Take the Brain Tour